
Understanding the past can help pave a path to future care.
- Skin failure or skin changes associated with dying are a recognized factor in skin breakdown, particularly toward end of life, but also with acute, chronic, and dermatologic conditions.
- No universal agreement exists among clinicians as to how skin failure develops, manifests, and progresses.
- The Braden Scale should be performed on all patients at risk to ensure optimum evidence-based practice to prevent skin breakdown.
- More research is needed to understand the phenomenon of skin failure, including the use of technologies such as long-wave infrared technology.
Learning Objectives
- Explain skin failure and skin changes at the end of life.
- Describe skin failure definitions over time.
- Discuss recent technological advances in skin assessment.
The author, planners, and peer reviewers of this CNE activity have disclosed no relevant financial relationships with any commercial companies pertaining to this activity. See the last page of the article to learn how to earn CNE credit.
Expiration: 10/1/26
Kennedy terminal ulcer. Kennedy lesion. Skin failure. Skin changes at life’s end. Terminal ulcers. Trombley-Brennan terminal tissue injury. End-stage skin. Skin changes associated with dying. Decubitus ominosus. Unavoidable pressure injuries. No matter what you call it, the question remains: Is skin failure a form of pressure injury or a separate phenomenon with a fundamentally different etiology?
As we age, our bodies become more subject to frailty, illness, weakness, and morbidity. Frailty frequently is defined as an aging-related syndrome of physiological decline, characterized by marked vulnerabilities to adverse health outcomes. We use the Braden Scale, an evidence-based pressure injury risk assessment tool, to predict the risk of skin breakdown and to explore functional and nutritional status. It guides clinical practice to prevent skin breakdown. However, with true age-related frailties, these efforts may be in vain. Skin is an organ, and similar to other organs—heart, liver, kidneys—we can’t dispute the possibility of its failure.
Consistent interest in skin failure has focused on clinical, ethical, and regulatory aspects, and has policy and legal ramifications. Although we most frequently speak of skin failure as an end-of-life event, it also can occur in relation to certain life-threatening conditions or severe illness. Experts continue to debate terminology, definitions, presentations, etiologies, and how skin failure (if that’s what you choose to call it) evolves and manifests.
The following historical perspective reviews the continuing evolution of our understanding of skin failure so we can best care for patients and manage their symptoms.
Ancient Greeks and Romans: Skin as a “surface envelope”
Ancient Greeks and Romans considered skin as something external, superficial, and superfluous, insisting on the notion of it as a “surface envelope.” Early evidence of pressure injuries has been found in Egyptian mummies dating back 5,000 years. For this reason, according to Santoro, the Ancients considered the skin to not be a “bearer of good news,” and that “the suffering of sickness and old age had emptied (it) of everything that made it alive and vital: pellis (animal hide) and cutis (human skin) merely represented the inert and insensitive matter of a body that had already been delivered to death.”
16th to 17th century: Skin appreciation
In 1563, Andries van Wesel’s publication of De humani corporis fabrica, gave skin, as the first barrier to be incised on the dissection table, some of the attention it deserves. He discovered new anatomical facts and revealed them to the world. van Wesel regarded skin as a “halfway house between flesh and nerves.” In the 17th century, the arrival of the microscope allowed scientists and clinicians better visualization, which increased their appreciation for the complex, layered elements and structures of the skin.
Mid-1800s: Decubitus ominosus
Charcot, a celebrated French neurologist, believed in the “neurotrophic theory” of decubitus (an old term derived from “lying down”) development, which held that damage to the central nervous system led directly to decubitus occurrence. He observed that many patients who developed skin breakdown, particularly with eschar on their buttocks, died soon afterward. He called it “decubitus ominosus.” Charcot’s drawings of this phenomenon, which include a butterfly shape as well as a unilateral presentation, mirror current pictures of Kennedy lesions. He also described neurologic disorders, such as Parkinson’s disease, multiple sclerosis, amyotrophic lateral sclerosis, and Charcot foot.
1980s: Kennedy lesion
Fast forward to the 1980s, when Karen Lou Kennedy, a nurse practitioner in a 500-bed mid-Western long-term care facility, observed that some residents rapidly developed skin breakdown, usually on their buttocks, and died within 6 weeks to months. She described the breakdown as red, yellow, or black pear-shaped purpuric areas on bony prominences, particularly on the sacrum. They appeared suddenly and when death was imminent.
Kennedy’s 1989 5-year retrospective study in a nursing home showed that 55.7% of people who died with a pressure injury died within 6 weeks of onset. A Kennedy terminal ulcer (now called Kennedy lesion), sometimes occurs so rapidly that it’s called a “3:30” lesion—it’s not present at the beginning of a nurse’s shift, but intact skin discoloration doubles in size quickly. The life expectancy of a patient with a 3:30 lesion could be as short as 8 to 24 hours.
1990s: Dermatology definition
In dermatology, skin failure, a term introduced by Irvine, describes severe skin conditions such as erythroderma, burns, pemphigus, Stevens-Johnson syndrome, and toxic epidermal necrolysis. The term equates it with the morbidity and mortality of other organ failures, such as the heart, kidney, and liver. He defined skin failure as a loss of normal temperature control and an inability to maintain core temperature and prevent percutaneous loss of fluid, electrolytes, and protein. This imbalance allows the penetration of foreign materials. The level of skin dysfunction prevents normal homeostasis and requires clinical intervention.
1991: Ethical considerations
La Puma advocated for ethical considerations when devising Agency for Health Care and Policy Research (now Agency for Healthcare Research and Quality) guidelines. He suggested identifying and acknowledging long- and short-term goals for patients with irreversible risk factors. In describing skin as the largest organ of the body, he noted that if other major organs show signs of failing, then skin failure also may occur. He asked why we view a pressure injury as an indication of inadequate healthcare when symptoms of heart or lung disease aren’t. He saw the development of a pressure injury as a potential sign of physical decline and mortality.
2006: Skin failure classification
In 2006, Langemo and Brown proposed a broader perspective of skin failure, and classified it as either acute, chronic, or end of life. Overall, they defined skin failure as caused by hypoperfusion that occurs at the same time as severe dysfunction or failure of other organs. (See Skin failure classification.)
Skin failure classification
Langemo and Brown classified skin failure as acute, chronic, and end-stage.
- Acute skin failure occurs in conjunction with an extended critical illness in which a patient, usually in the intensive care unit, experiences significant risk factors for pressure injury development, including sensory deprivation, immobility, hypoperfusion, anemia, and malnutrition.
- Chronic skin failure occurs as a result of hypoperfusion concurrent with an ongoing, chronic disease state. Ultimately, the skin and underlying tissue collapse when multiple failing organ systems can no longer provide support.
- End-stage skin failure occurs at end of life. As organs fail, the body redirects blood away from the skin in an attempt to maintain organ function. The result can include large and unusual presentations of skin failure.
2009: End of life
In 2009, a consensus panel of experts conceived of the Skin Changes at Life’s End (SCALE) to recognize possible skin alterations that occur during the dying process. The SCALE document proposes that the skin isn’t impervious to dysfunction at the end of life and may include varying degrees of skin and tissue damage, including pressure injuries. Increased skin hypoxia resulting from reduced oxygen availability to the tissues reduces the body’s ability to use nutrients necessary for maintenance and repair. The panel published ten consensus statements along with the following general conclusions:
- The skin is the body’s largest organ and like any other organ is subject to a loss of integrity.
- Our current comprehension of skin changes that can occur at life’s end is limited.
- The SCALE process is insidious and difficult to determine prospectively.
- Additional research and expert consensus are necessary.
- Contrary to popular myth, not all pressure injuries are avoidable.
2012: Trombley-Brennan terminal tissue injury
A group of palliative care nurses noted the rapid onset of skin changes characterized by bruising on nonbony prominences in their end-of-life patients, which frequently were mischaracterized as pressure injuries. Median time from identification of skin changes to death was 36 hours. Injury hallmarks included rapid evolution, sudden enlargement and progression, appearance in areas with little to no pressure (such as the shins and thighs), and bilateral mirror images of each injury. Frequently, the injuries presented as linear striations on lower extremities or on the thoracic and lumbar spine, were non-blanching, and appeared deep reddish-purple. A 2019 study by Brennan and colleagues, which adds 86 new patients, builds on these results
2017: Expanding the definition
Levine expanded on the concept and definition of skin failure, defining it as the state “in which tissue tolerance is so compromised that cells can no longer survive in zones of physiologic impairment such as hypoxia, local mechanical stresses, impaired delivery of nutrients, and buildup of toxic metabolic byproducts.” External pressure and stretching of not only skin but also underlying tissues over bony prominences, such as occurs in pressure areas, can contribute to or cause skin failure.
2020: COVID-19 skin manifestations
The National Pressure Injury Advisory Panel (NPIAP) advises wound care providers to consider whether purpuric skin changes are forms of deep tissue injury or skin failure. COVID-19 creates systemic coagulopathy with microvascular occlusion, which may lead to stroke and pulmonary embolism. This accelerated clotting process also appears to involve the skin. Skin lesions associated with COVID-19 hypercoagulopathy have varied appearance and patterns, which include purpura in the skin, which may become necrotic and frequently occur in areas not exposed to pressure.
2020: SFCIS
In a small study that included 52 patients in acute care who experienced skin breakdown before death, Hill and Petersen found that the Skin Failure Clinical Indicator Scale (SFCIS) helped to distinguish between skin failure and pressure injury. The scale includes the following factors: serum albumin level <3.5 mg/dL (P = .07), impaired blood flow (P = .05), presence of sepsis/multiorgan dysfunction syndrome (P = .001), vasopressor/inotrope use (P = <.001), and mechanical ventilation (P = .06). Ultimately, the SFCIS correctly identified 83.7% of patients as having probable skin failure.
2021: NPIAP conference
In the fall of 2021, NPIAP convened a conference to discuss skin failure related to end of life, focusing on consensus around terminology and drawing attention to how little scientific research exists regarding the condition. The conference addressed the common physical manifestations of skin failure, how it evolves, and how, with little diagnostic guidance, clinicians can recognize it. Attendees also considered whether skin breakdown is unavoidable. At the end of the conference, the group reached consensus on changing the terminology from “skin failure” to “skin change (associated with dying).”
Histologically, as described in a NPIAP press release, specimens from embalmed cadavers with dark intact skin showed the presence of lesion changes. However, their appearance differs from Stage 1 or deep-tissue pressure injuries (DTPI). Long-wave infrared thermography (LWIT) imaging of hospice patients distinguished DTPI from non-pressure related injury, such as skin failure. Temperature differentials under an area of pressure showed either a warmer area (>1.2° C), which indicates inflammation, or a cooler area (<1.2° C), which indicates ischemia. In the absence of a thermal anomaly, discoloration is presumed to be superficial and most likely the result of causes other than pressure, such as skin failure, Kennedy lesion, bleeding, or vasopressor use.
2022: Expanded definition, proposed model
Levine and colleagues acknowledged the difficulties still surrounding the concept of skin failure, including no conceptual consensus across clinical entities and no common recognition by all providers and regulatory bodies. We still have no universally accepted definition and no agreement on clinical manifestations or identified biomarkers. Levine and colleagues reviewed pathophysiologic factors such as hypoperfusion, hypoxia, inflammation, increased vascular permeability and edema, as well as conditions such as multiple organ dysfunction syndrome, malnutrition, and immunocompromise. Ultimately, the authors concluded that clarifying the pathophysiology of skin failure will significantly aid clinical care, quality measurement, and healthcare policy.
2022–2023: Advanced technology
Recent research with LWIT has determined that, contrary to pressure injuries, no temperature change occurs in the skin of a Kennedy lesion in the first 24 hours of discoloration. In a lecture at the Wound, Ostomy and Continence Nurses Society 2022 National Conference, Kennedy and Ritter reiterated the skin temperature differences in areas of pressure. This supports the assertion that true Kennedy lesions are not pressure related.
Technologies such as LWIT may herald a new era of understanding with better diagnostics to differentiate pressure injury from other types of skin breakdown. This could lead to earlier identification of pressure injuries with more effective prevention and treatment and improved outcomes, as well as recognition of the unavoidability and futility in the case of skin failure. Further research could provide needed objective data for differentiating skin failure from DTPI. (See LWIT in action.)
LWIT in action
Long-wave infrared thermography (LWIT) can aid identification of pressure injuries (PIs) and Kennedy lesions via detection of relative temperature differential (RTD). The following images depict normal, PI, and Kennedy lesion visualization and thermal imaging.
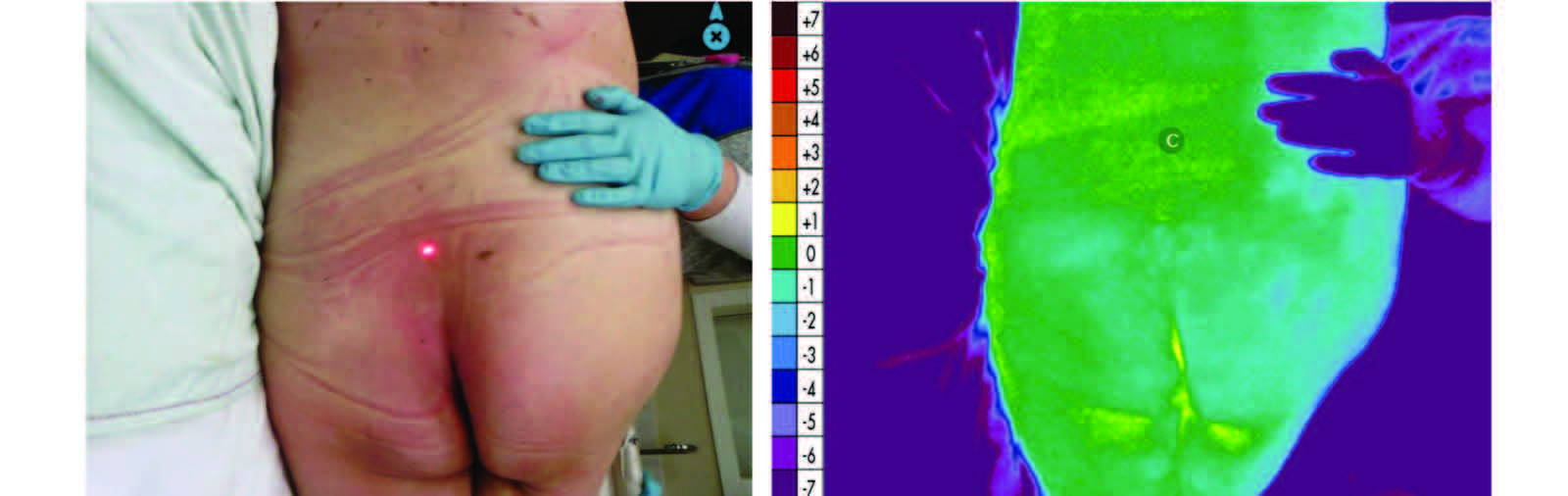
Intact skin: Photograph shows no skin discoloration. The thermal image shows a sprinkling of green and yellow, which indicates a normal RTD range (≤+1.1° C ≥-1.1°C with light blue, green, and yellow on the thermal color scale).
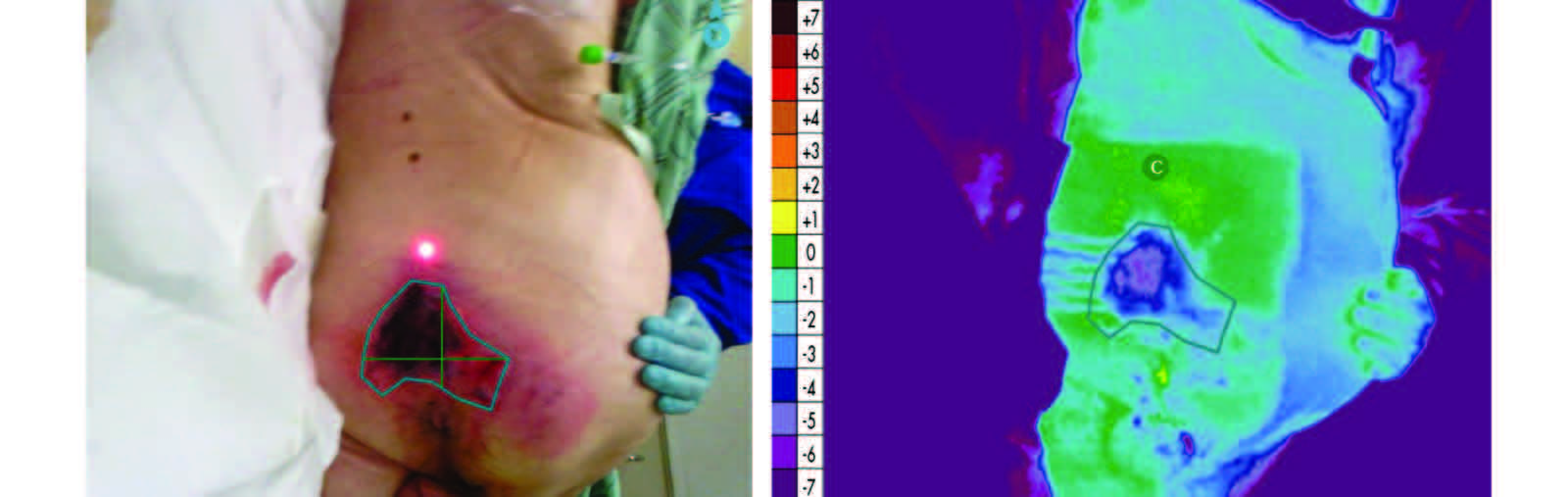
Pressure injury: Photograph shows a wound with eschar. The thermal image shows a localized and demarcated area with an abnormally low RTD of -3.5° C with blue and purple color outside of the normal RTD range. The abnormal RTD range is ≥+1.2° C (orange/red) and ≤-1.2°C (blue/purple).
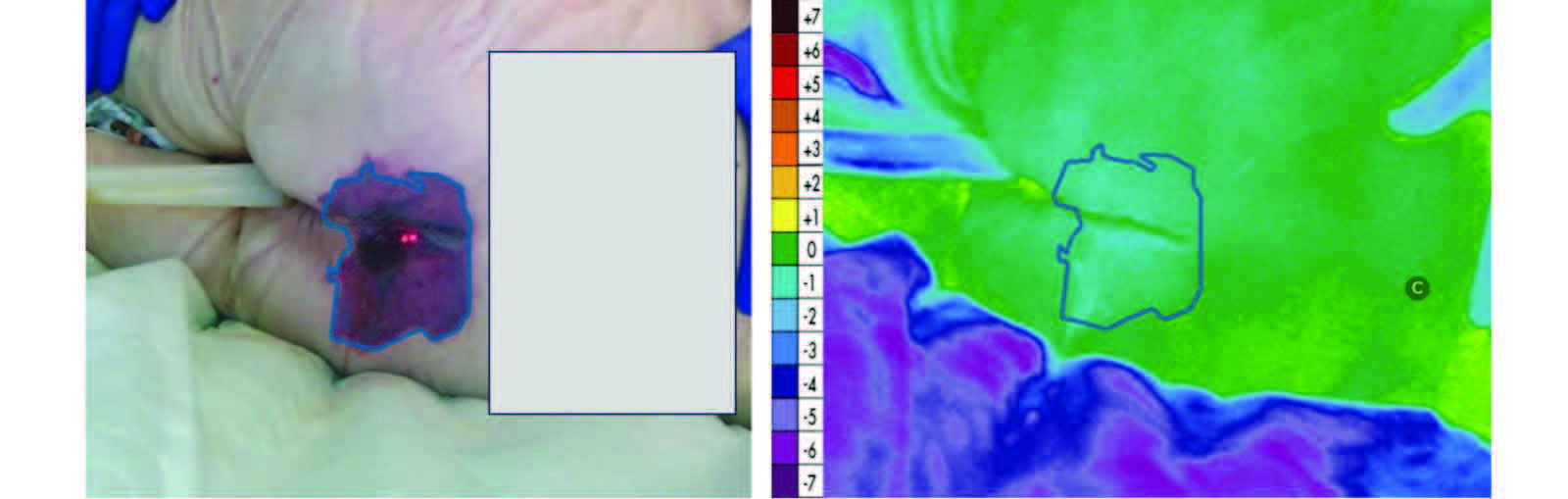
Kennedy lesion: The thermal image shows diffuse sprinkling of green and light blue (within the normal RTD range) in the presence of wound (photograph).
Images courtesy of WoundVision, LLC. Text adapted from Kennedy-Evans KL, Vargo D, Ritter L, Adams D, Koerner S, Duell E. Early skin temperature characteristics of the Kennedy lesion (Kennedy terminal ulcer). Wound Manag Prev. 2023;69(1):14-24.
Finding answers
Many unknowns and disagreements related to skin failure and skin changes at end of life exist, with important and significant ethical, clinical, policy, regulatory, reimbursement, and legal consequences.
La Puma raised important ethical concerns about the wisdom of aggressive interventions in the face of obvious organ failure. This can be a perilous time for healthcare providers because of the difficulty of explaining futility to family members, who sometimes expect perfect outcomes despite patient status. Skillful communication and empathy can help prevent litigation.
Clinically, wound care providers must find common ground, knowledge, and terminology to provide evidence-based care in the most ethical way possible. We also must be cognizant of our scarce resources, and use them efficiently yet empathetically. Appropriate care requires data-driven evidence supported by sound research, with interdisciplinary consensus.
Similarly, good healthcare policy should be guided by rigorous research, with strong advocacy by wound care providers and organizations in collaboration with policy makers. We must advocate for policies consistent with evidence-based care as well as adequate reimbursements and coding.
In terms of regulation and reimbursement, regulators and payors, such as the Centers for Medicare and Medicaid Services, still penalize acute care facilities for hospital-acquired pressure injuries. However, they allow for the possibility of unavoidable pressure injuries in long-term care as long as the facility takes adequate prevention steps, including clinical evaluation, evidence-based interventions, patient monitoring, and revised strategies as needed. These same regulations could be applied to acute care settings.
Legally, the shocking nature of pressure injuries and skin failure can add substantially to U.S. healthcare costs. Pressure injuries represent the lion’s share of medical malpractice litigation. The defense must be able to show that the morbidity and mortality associated with skin breakdown, particularly at the end of life, is attributable to uncontrollable intrinsic factors. Thoughtful communication with family members can offer comfort and understanding of the natural death process. Healthcare providers must show, however, that they’ve met all standards of care related to skin breakdown prevention and treatment.
Clinicians have no firm guidelines, data, or criteria to direct their practice when it comes to recognizing and diagnosing skin failure and skin changes associated with dying. Are pressure injuries clinically different from skin failure with different clinical implications? With continued interest in the subject, advanced diagnostic tools, and more research to aid understanding, we’ll have clearer answers to this dilemma.
Heidi H. Cross is a wound and ostomy nurse practitioner at HHC Wound Care Consulting in Syracuse, New York, CNY Surgical Physicians in Syracuse, and the University of Rochester Strong Memorial Hospital in Rochester, New York.
American Nurse Journal. 2023; 18(10). Doi: 10.51256/ANJ102306
References
Ayello EA, Levine JM, Langemo D, Kennedy-Evans KL, Brennan MR, Sibbald RG. Reexamining the literature on terminal ulcers, SCALE, skin failure, and unavoidable pressure injuries. Adv Skin Wound Care. 2019;32(3):109-121. doi:10.1097/01.ASW.0000553112.55505.5f
Black J, Cuddigan J, Capasso V, et al. on behalf of the National Pressure Injury Advisory Panel. Unavoidable pressure injury during COVID-19 crisis: A position paper from the National Pressure Injury Advisory Panel. 2020. cdn.ymaws.com/npiap.com/resource/resmgr/white_papers/Unavoidable_in_COVID_Pandemi.pdf
Black J, Cuddigan J, and members of the National Pressure Injury Advisory Panel Board of Directors. Skin manifestations with COVID-19: The purple skin and toes that you are seeing may not be deep tissue pressure injury. An NPIAP White Paper. 2020. cdn.ymaws.com/npiap.com/resource/resmgr/white_papers/COVID_Skin_Manifestations_An.pdf
Brennan MR, Thomas L, Kline M. Prelude to death or practice failure? Tombley-Brennan terminal tissue injury update. Am J Hosp Palliat Med. 2019;36(11):1016-9. doi: 10.1177/1049909119838969
Dalgleish L, Campbell J, Finlayson K, et al. Understanding skin failure: A scoping review. Adv Skin Wound Care. 2021;34(10):542-50. doi:10.1097/01.ASW.0000755844.87283.20
Hill R, Petersen A. Skin failure clinical indicator scale: Proposal of a tool for distinguishing skin failure from a pressure injury. Wounds. 2020;32(10):272-8.
Irvine C. ‘Skin failure’—A real entity: Discussion paper. J R Soc Med. 1991;84(7):412-3. doi:10.1177/014107689108400711
Kennedy KL. The prevalence of pressure ulcers in an intermediate care facility. Decubitus. 1989;2(2):44-5.
Kennedy KL, Ritter L. The science catches up with the Kennedy terminal ulcer. Lecture presented at: 2022 Wound, Ostomy and Continence Nurses Annual Conference; June 6, 2022; Fort Worth, TX.
Kennedy-Evans KL, Vargo D, Ritter L, Adams D, Koerner S, Duell E. Early skin temperature characteristics of the Kennedy lesion (Kennedy terminal ulcer). Wound Manag Prev. 2023;69(1):14-24.
Langemo DK, Brown G. Skin fails too: Acute, chronic, and end-stage skin failure. Adv Skin Wound Care. 2006;19(4): 206-11. doi: 10.1097/00129334-200605000-00014
La Puma J. The ethics of pressure ulcers. Decubitus. 1991;4(2):43-44.
Levine JM. Historical perspective: The neurotrophic theory of skin ulceration. J Am Geriatr Soc. 1992;40(12):1281-3. doi:10.1111/j.1532-5415.1992.tb03656.x
Levine JM. Historical perspective on pressure ulcers: The decubitus ominosus of Jean-Martin Charcot. J Am Geriatr Soc. 2005;53(7):1248-51. doi:10.1111/j.1532-5415.2005.53358.x
Levine JM. Unavoidable pressure injuries, terminal ulceration, and skin failure: In search of a unifying classification system. Adv Skin Wound Care. 2017;30(5):200-2. doi:10.1097/01.ASW.0000515077.61418.44
Levine JM, Delmore B, Cox J. Skin failure: Concept review and proposed model. Adv Skin Wound Care. 2022;35(3):139-48. doi:10.1097/01.ASW.0000818572.31307.7b
National Pressure Injury Advisory Panel. NPIAP tackles issue of skin changes in actively dying patients. December 17, 2021. npiap.com/news/590421/NPIAP-Tackles-Issue-of-Skin-Changes-CM, in-Actively-Dying-Patients.htm
Santoro R. Skin over the centuries. A short history of dermatology: physiology, pathology and cosmetics. Med Histor. 2017;1(2):94-102.
Sibbald RG, Krasner DL, Lutz J, et al. SCALE: Skin changes at life’s end. Final consensus statement: October 1, 2009. Adv Skin Wound Care. 2010;23(5):225-36. doi:10.1097/01.ASW.0000363537.75328.36
Trombley K, Brennan MK, Thomas L, Kline M. Prelude to death or practice failure? Trombley-Brennan terminal tissue injuries. Am J Hosp Palliat Med. 2012;29(7):541-5. doi:10.1177/1049909111432449
Vargo D. Differentials made easy by assessing the temperature of the skin and soft tissue with long-wave infrared thermography (LWIT). Lecture presented at the National Pressure Injury Advisory Panel Annual Conference; March 10-12, 2021; Washington, DC.
Walston JD. Frailty. UpToDate. June 12, 2023. uptodate.com/contents/frailty
Key words: skin failure, pressure injury, end of life, Kennedy lesion

















4 Comments. Leave new
I am skin Nurse champion at my job.
I loved learning the historical perspectives and the current concepts of SKIN FAILURE: a historical perspective. It contributes to my proper assessment, goal-setting, formulation of care and intervention, as well as measurement of outcomes. Thank you.
I have seen the Kennedy’s ulcer frequently in hospice patients.
The skin failure is interesting and needs much research.
Thanks,
Zerlene