

Implement protocols for early identification and management.
Takeaways:
- Sepsis has received much attention recently, but the pediatric population is missing from many of these discussions.
- Increased nursing knowledge about sepsis recognition, management, and emergency care can improve outcomes for these patients.
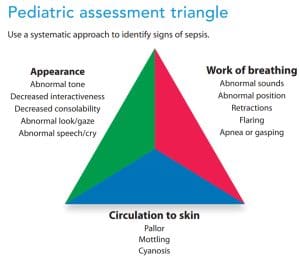
- The pediatric assessment triangle can aid early identification of sepsis signs and symptoms.
Liz Borough* calls emergency medical services when her son, Owen, a 28-day-old infant, becomes unresponsive. He requires resuscitation and is taken to the emergency department (ED) at the local hospital. The ED nurse notes Owen’s pale skin and that he has no other vital sign abnormalities. The ED physician admits Owen to the pediatric care unit for observation.
Overnight, Owen develops a fever of 101.2°F (38.4°C). The nurse, Robert Conner, completes a thorough assessment, noting capillary refill >3 seconds. Robert asks Ms. Borough if she’s noticed any changed behavior in Owen. She says that her son has been fussier than usual and not easy to console. Using the pediatric assessment triangle, Robert recognizes these as signs and symptoms of sepsis and calls the pediatric hospitalist. (See Pediatric assessment triangle.)
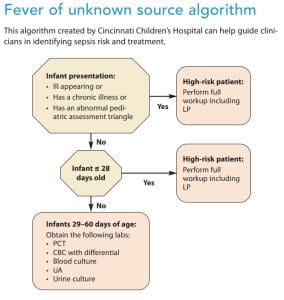
The hospitalist uses an algorithm (such as the Cincinnati Children’s Fever of Unknown Source) to conclude that Owen is at high risk for a serious bacterial illness. She outlines the plan of care, which includes a complete septic workup with catheterized urine collection, lumbar puncture, blood work, I.V. fluids, and broad-spectrum antibiotics. The hospitalist thanks Robert for his good catch and attention to detail. (See Fever of unknown source algorithm.)
Identifying sepsis
Typically, when a patient between 0 and 60 days old presents with a fever, the source is viral. However, nurses must follow current guidelines for appropriate management, and healthcare leaders should implement protocols and order sets to ensure implementation of evidence-based assessments and treatment.
Assessment
Infants, such as Owen, at presumed high risk for sepsis should receive a complete sepsis assessment, including blood work (pro-calcitonin [PCT], complete blood count, basic metabolic panel, and blood cultures), lumbar puncture to analyze cerebral spinal fluid (CSF), and catheterization for urine analysis, culture, and sensitivity. Tests appropriate for the initial assessment include protein, glucose, culture and gram stain, cell count, and differential. One tube of blood should be labeled and held in the lab in the event additional studies, such as for herpes simplex virus (HSV), are required.
In the past 20 years, the incidence of HSV in the United States has increased to 1 in 2,000 live births. HSV is most frequently transmitted during delivery, but postnatal transmission also occurs from family and caregivers. The incubation period ranges from 2 days to 2 weeks. HSV should be a consideration for neonates (between birth and approximately 6 weeks of age) who present with fever, a vesicular rash, or abnormal CSF findings.
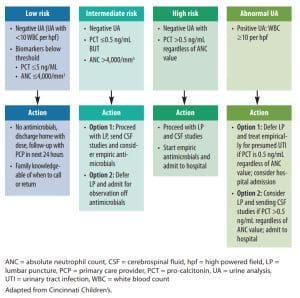
Make sure to follow your specific lab’s reference range for abnormal values as they may differ. In pediatric patients, a PCT >0.5 ng/mL is considered indicative of a serious bacterial infection. The higher the PCT, the greater the sepsis severity. However, PCT can yield false positives and should be combined with clinical assessment. Patients suspected to have sepsis require prompt antibiotic therapy, but blood cultures should be drawn before administering antibiotics. Obtain cultures immediately to avoid treatment delays. If you encounter difficulty obtaining blood cultures, contact the provider immediately. Urine analysis in patients between 0 and 60 days old with a white blood cell count >10 is considered a positive result that requires treatment.
Group B Streptococcus (GBS), a leading cause of sepsis in infants, has no effective preventive strategy. Early-onset GBS sepsis typically occurs between birth and 6 days; late-onset GBS sepsis occurs in infants up to 90 days of age. All newborn infants should be assessed for their risk of developing GBS sepsis using the Neonatal Early-Onset Sepsis Calculator. Knowing maternal GBS status is important for infants presenting with clinical signs of sepsis, but late-onset GBS occurs in infants regardless of maternal status during pregnancy.
Treatment
Owen’s initial treatment includes broad-spectrum antibiotics. Patients showing signs of septic shock should receive antibiotics within 1 hour. Patients who have sepsis without shock should receive antibiotics within 3 hours. Owen received his assessment and antibiotics within 1 hour of identification. In addition, the provider ordered an empiric therapy regimen of ampicillin, a third-generation cephalosporin (alternatively the provider could have prescribed gentamicin), and maintenance I.V. fluids with lactated ringers. Pediatric patients with hypotension should receive between 10 to 20 mL/kg of I.V. fluids within the first hour, with or without pediatric intensive care availability. Because Owen didn’t have hypotension, the provider didn’t order a fluid bolus. Fluid boluses aren’t routinely recommended in hospitals without a PICU because they may not have the resources to manage treatment complications.
Owen receives a final diagnosis of urinary tract infection after his urine analysis shows 10 plus white blood cells and his culture and sensitivity indicate the presence of Escherichia coli. To cover the identified bacteria, the provider modifies Owen’s antibiotic regimen to include ceftriaxone.
Nursing implications
Sepsis has received a great deal of attention recently, but the pediatric population is missing from many of these discussions. Increased nursing knowledge about sepsis recognition, management, and emergency care can improve outcomes for these patients. Many early warning signs of pediatric sepsis go unrecognized, especially outside of pediatric tertiary care centers. According to the Emergency Medical Services for Children Innovation and Improvement Center, approximately 70% of EDs in the United States see fewer than 15 pediatric patients per day. This low volume creates challenges to establishing pediatric quality metrics and performance standards.
Early and accurate diagnosis of pediatric sepsis, a leading cause of morbidity, mortality, and healthcare utilization for children worldwide, remains challenging. To ensure prompt sepsis recognition and treatment, ED nurses must have the knowledge, tools, and equipment necessary to care for pediatric patients of all ages. Standardized screening and early-warning systems aid in early treatment and reduce morbidity and mortality.
In addition, relationship-based nursing practice allows parents and guardians to act as integral members of the care team. Intentional listening and addressing caregiver concerns has the potential to speed sepsis recognition and response. (See What nurses can do.)
What nurses can do
This checklist, designed to empower nurses to drive the evidenced-based changes necessary to improve sepsis recognition and management in pediatric patients, serves as a starting point for improving patient safety. The steps can be completed in any order.
Get involved.
- Commit to investing time in pediatric sepsis identification and management as part of your hospital’s nursing professional advancement program or clinical ladder.
- Work with your organization’s sepsis coordinator to implement a quality improvement program that acknowledges the differences between adult and pediatric management and includes standardized screening and procedures for pediatric patients identified as at-risk for sepsis.
Set measurable quality improvement goals.
- Create a dashboard and report pediatric sepsis data to pediatric and emergency care providers as well as organizational leadership.
Implement the Neonatal Early-Onset Sepsis Calculator.
- The interactive Kaiser Permanente calculator assesses newborn infants born ≥34 week’s gestation for their risk of developing early-onset sepsis.
- Many electronic health record (EHR) systems can automate use of the Early Onset Sepsis Calculator or it can be accessed at neonatalsepsiscalculator.kaiserpermanente.org
Implement the pediatric assessment triangle.
Complete the National Pediatric Readiness Survey.
- This survey from the Pediatric Readiness Project helps emergency departments identify gaps in their readiness to care for pediatric patients.
- The survey can be accessed at pedsready.org.
Create standardized protocols for pediatric sepsis management.
- Bundled protocols or order sets can help address the unique needs of pediatric patients seeking emergency care.
- Consider developing separate protocols for patients 0 to 60 days of age and ≥61 days.
- Refer to the Society of Critical Care Medicine’s (SCCM) Surviving Sepsis Campaign Guidelines to create protocols.
Establish a pediatric emergency care coordinator role.
- Refer to the American Academy of Pediatrics policy statement for evidence to support the role of a pediatric emergency care coordinator at your organization.
- The role includes responsibilities related to pediatric emergency care policies, training, and resources.
Encourage participation in state-level pediatric readiness programs.
Investigate state pediatric medical recognition program opportunities.
Develop an EHR pediatric early warning system.
- Request the addition of capillary refill, pulse strength, and hand and foot temperature assessments to pediatric nursing flowsheets. These are early warning signs for pediatric sepsis.
- Low blood pressure is a late sign of sepsis.
Weigh and record all pediatric patients in kilograms.
- This step can help prevent catastrophic drug dosing errors.
- In addition, include the patient’s weight in kilograms on all prescriptions.
Develop sepsis screening tools.
- Share these tools with colleagues as a resource to promote early recognition of pediatric sepsis.
Implement a standardized communication tool.
- Prompt communication of sepsis concerns aids quick treatment.
- Tools such as ISBARQ (introduction, situation, background, assessment, recommendation, and questions) can help ensure suspicions are shared effectively with providers.
Discuss molecular technology for pediatric blood cultures with laboratory leadership.
- Molecular methods speed microorganism identification and help predict susceptibility to antimicrobials.
- Perform a cost-vs-benefit analysis comparing the cost of implementing molecular technology in your hospital to the cost of sepsis (include pediatric data).
Implement an antibiotic stewardship program.
- If your facility already has a committee, ensure pediatric review and recommendations are shared.
Work with local emergency medical services (EMS) to determine pre-hospital pediatric readiness.
- The role of pre-hospital emergency care is critical in the continuum of care.
- EMS must address children’s unique needs.
Set realistic pediatric care improvement goals.
- For example, most community hospitals don’t have the resources (such as a pediatric intensive care unit) to manage sepsis complications (such as fluid overload). In that situation, the SCCM recommends maintenance fluids rather than bolus fluids.
- Design appropriate order sets and guidelines to fit your organization’s resources.
Start the change
Nurses should be empowered to speak up for patients through patient safety platforms. Hospital leadership can support inpatient and outpatient sepsis management across the continuum by implementing a comprehensive sepsis recognition and screening program for patients of all ages. Changes in pediatric sepsis management start with you.
Alysia Adams is nursing faculty at the University of Florida and the lead advanced practice provider at Ascension St. Vincent’s Riverside Hospital in Jacksonville, Florida. Ashley Lynch Denton is a nurse manager in the neonatal intensive care unit at Owensboro Health in Owensboro, Kentucky.
References
Bobillo-Perez S, Rodríguez-Fanjul J, Garcia IJ. Is procalcitonin useful in pediatric critical care patients? Biomark Insights. 2019;13:1177271918792244. doi:10.1177%2F1177271918792244
Cincinnati Children’s. Evidence-based care guideline for management of infants 0 to 60 days with fever of unknown source. May 7, 2019.
Downes KJ, Fitzgerald JC, Weiss SL. Utility of procalcitonin as a biomarker for sepsis in children. J Clin Microbiol. 2020;58(7):e01851-19. doi:10.1128%2FJCM.01851-19
Emergency Medical Services for Children Innovation and Improvement Center.
Puopulo K, Lynfield R, Cummings JJ. Management of infants at risk for Group B Streptococcal disease. Pediatrics. 2019;144(2):e20191881. doi:10.1542/peds.2019-1881
Weiss S, Peters MJ, Alhazzani W, et al. Surviving Sepsis Campaign international guidelines for the management of septic shock and sepsis-associated organ dysfunction in children. Pediatr Crit Care Med. 2020;21(2):e51-106. doi:10.1097/PCC.0000000000002198















1 Comment. Leave new
Thank you for this wonderful write up, it really helps me